We have already established that treating HIV is extremely difficult and that cells which have already been infected by the virus cannot be cured. Part of the reason that the disease is so difficult to treat is that the virus is so simple, which means there are not a lot of target sites for medicines. Another reason is that the structures that physically make up the virus are very similar to those in human cells, so if a drug is designed to attack these structures it will damage both the virus and the human host.
Perhaps a better strategy to control HIV is to prevent infection in the first place.
Prophylaxis
Prophylaxis are a type of medicine given to prevent diseases in people who are at high risk of contracting them. HIV drugs have a huge range of side effects that stem from the similarities between HIV and human cells. So, treatment with prophylaxis is not to be taken lightly and is reserved for those who are at high risk of contracting the disease. There are two main classes of prophylaxis: pre and post exposure. Pre-exposure treatment is given to people who will potentially be exposed to the virus, such as the sexual partner of someone who is HIV positive. The drugs must be taken correctly to be effective but due to the severe side effects cannot be taken indefinitely over a life-time and are prescribed for 3 months at a time. Post-exposure prophylaxis is a more intense treatment for people known to have been exposed to the virus, such as medical professionals that have been in direct contact with contaminated blood. This could include needle stick injuries or infected blood from a trauma patient getting onto a skin abrasion or mucous membrane of emergency staff.
Immunisation
Immunisation is a way of ‘training’ the body’s natural defence system to defend itself against a specific disease. Vaccines like the MMR are extremely effective in protecting individuals from the associated viral diseases (measles, mumps and rubella), as well as limiting the spread of the virus through communities. During immunisation people are injected with a non-disease-causing version of the virus or piece of the virus. This triggers a specific immune response in the person; this means that the body has a defence system ready to be quickly dispatched if the virus should ever enter the body. So why isn’t there an immunisation against HIV?
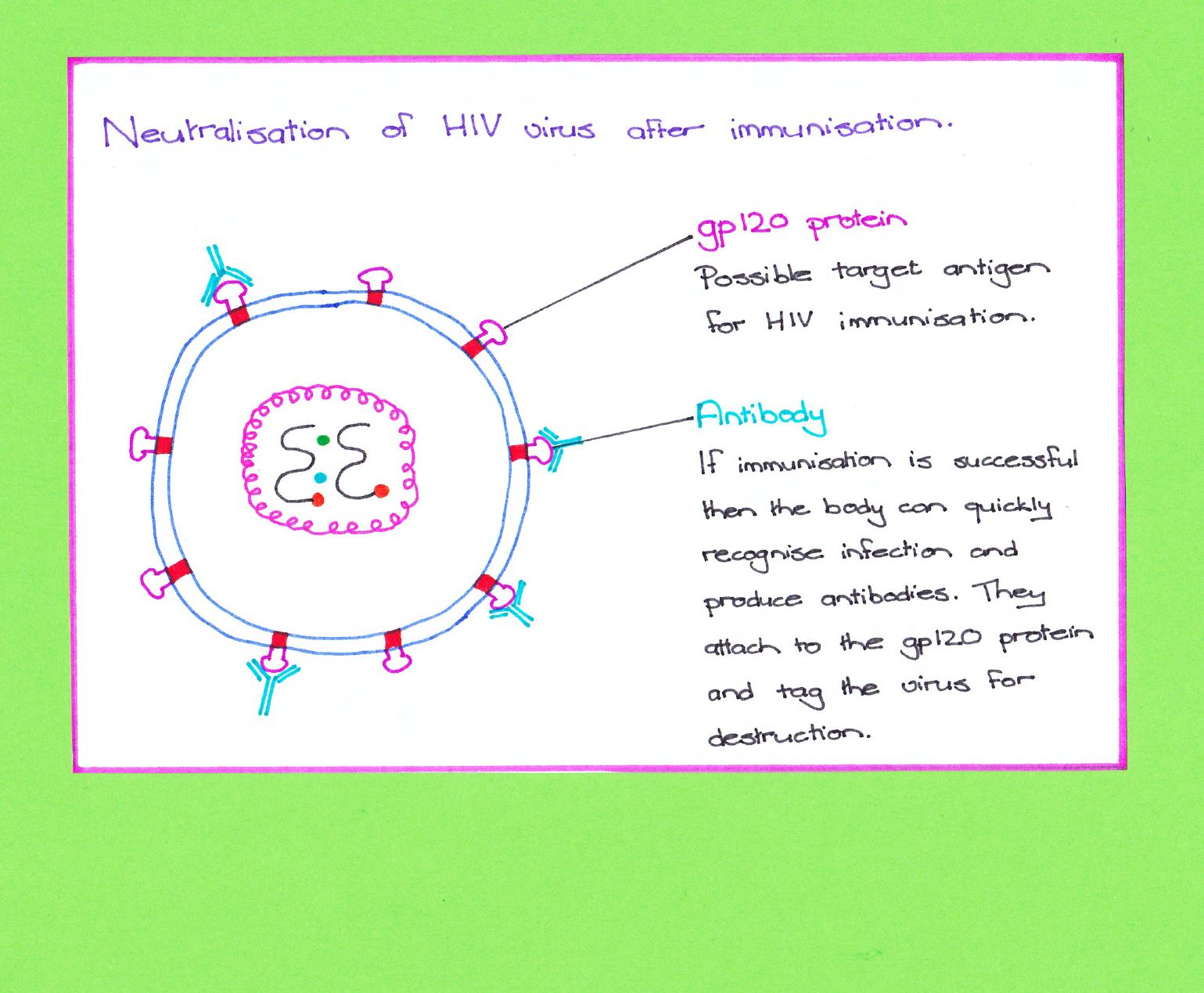
Immunisations rely on the target virus having a specific unique structure that can be used to trigger an immune response, this is called the antigen. The antigen is like a flag that the body is trained to recognise and destroy. The ideal HIV vaccine would contain an antigen present in all strains of the virus, it would trigger a maximum immune response while being safe and durable.
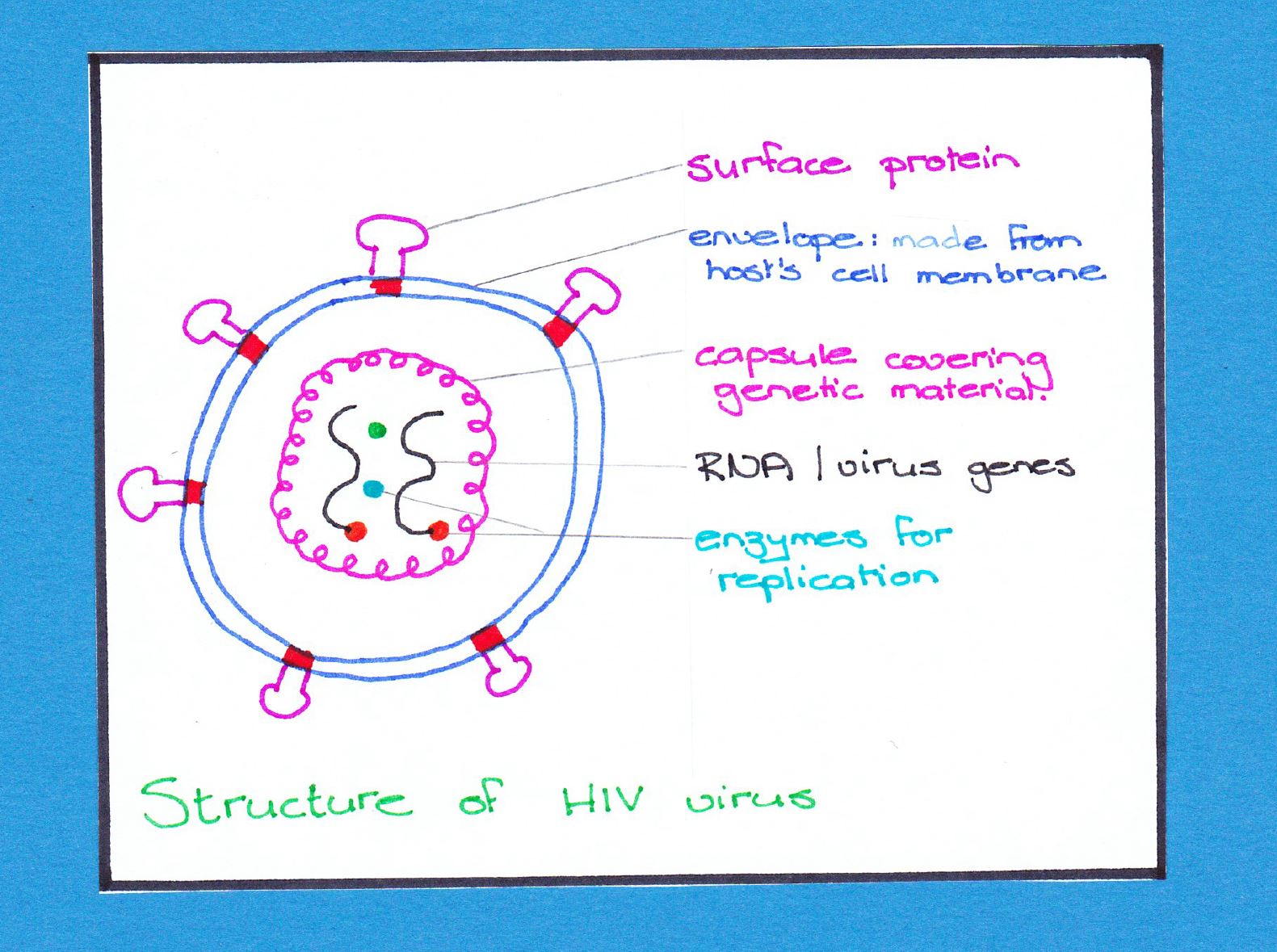
The problem with HIV is that it is such a small, simple and rapidly mutating virus. In addition to that it spends the majority of its time hidden inside human cells. When HIV leaves the human cell it is covered by an envelope, this has a protein on the surface of it called gp120. Gp120 is the protein that the HIV virus uses to attach to the human CD4 cells and infect them. This protein would be an ideal immunisation target (antigen). The downside is that the HIV virus has a genetic mechanism to change the structure of the Gp120 protein if it is recognised by the immune system. This rules out simply injecting the protein itself as a vaccine. A possible way around this is to take the HIV genes that code for the gp120 protein and insert them into a harmless virus, called a vector. The vector would then produce the gp120 proteins but would remain harmless to the host. Immunisation with the gp120 producing vector virus would expose the gp120 protein to the immune system leading to theoretical immunity against HIV. The is being clinically tested, as well as several other immunisation strategies.
The medical and biotechnical research in this area is incredible. However, the strategy that is the most effective in combating the spread of HIV is public education and avoidance of high risk behaviour such as unprotected sex and needle sharing.